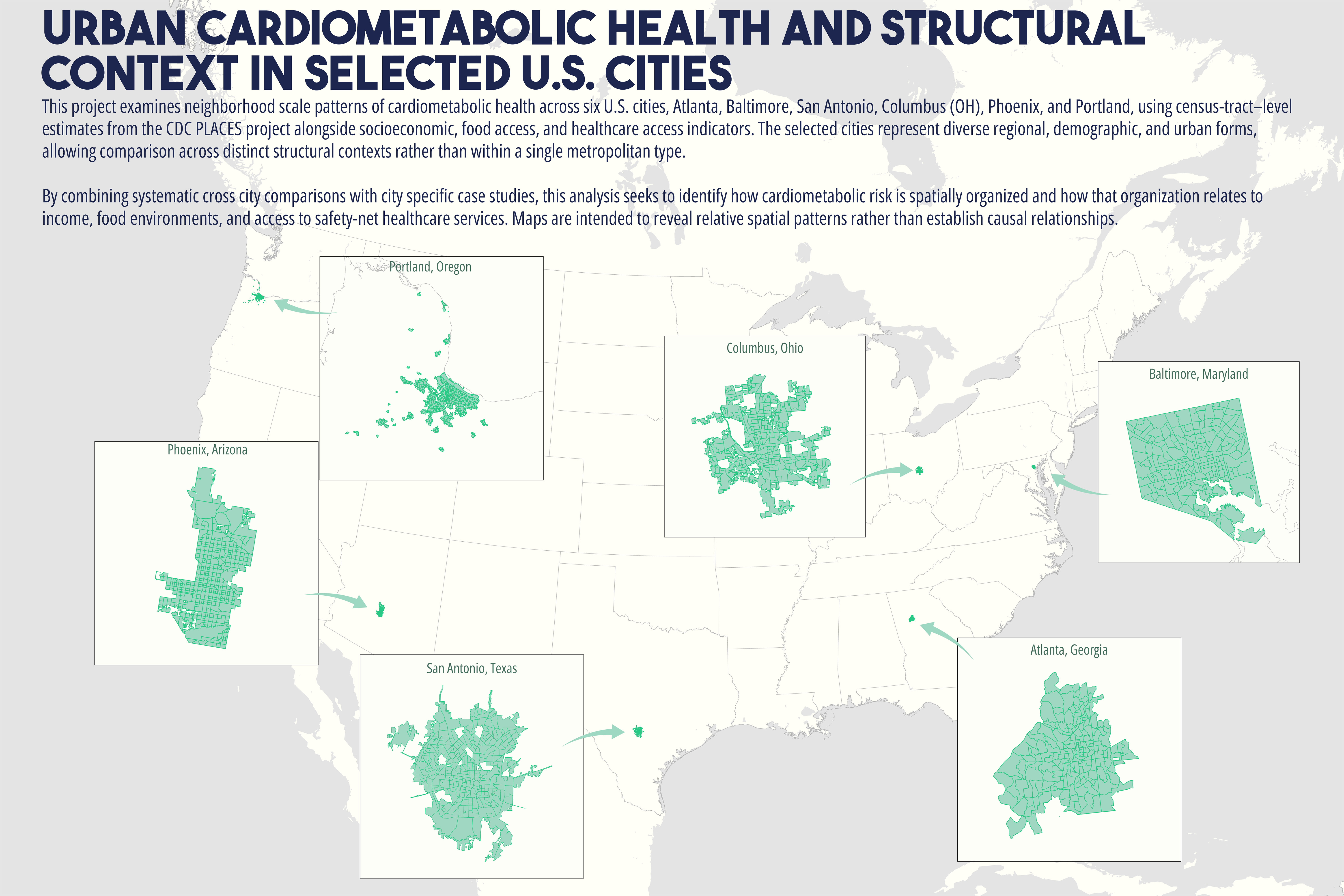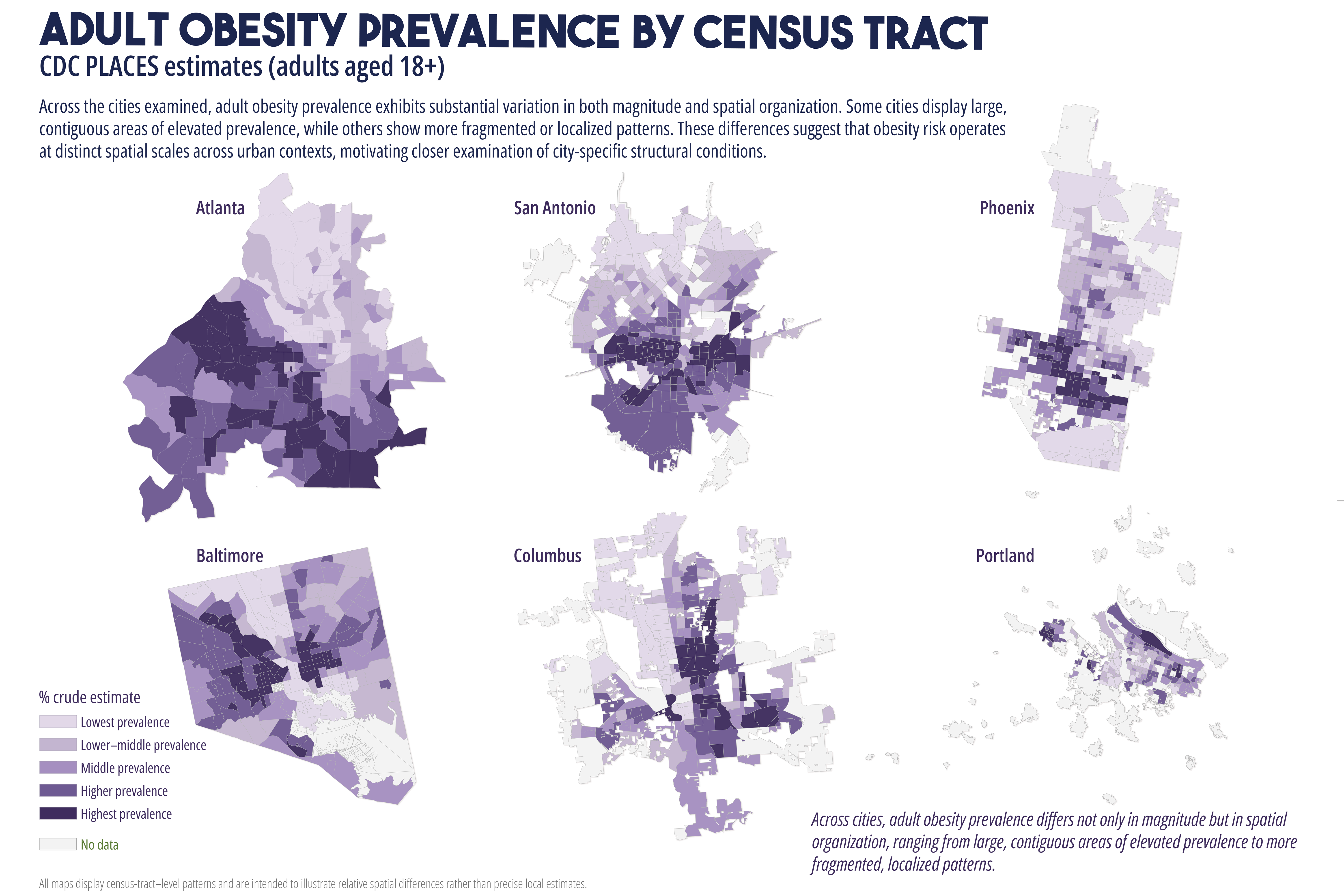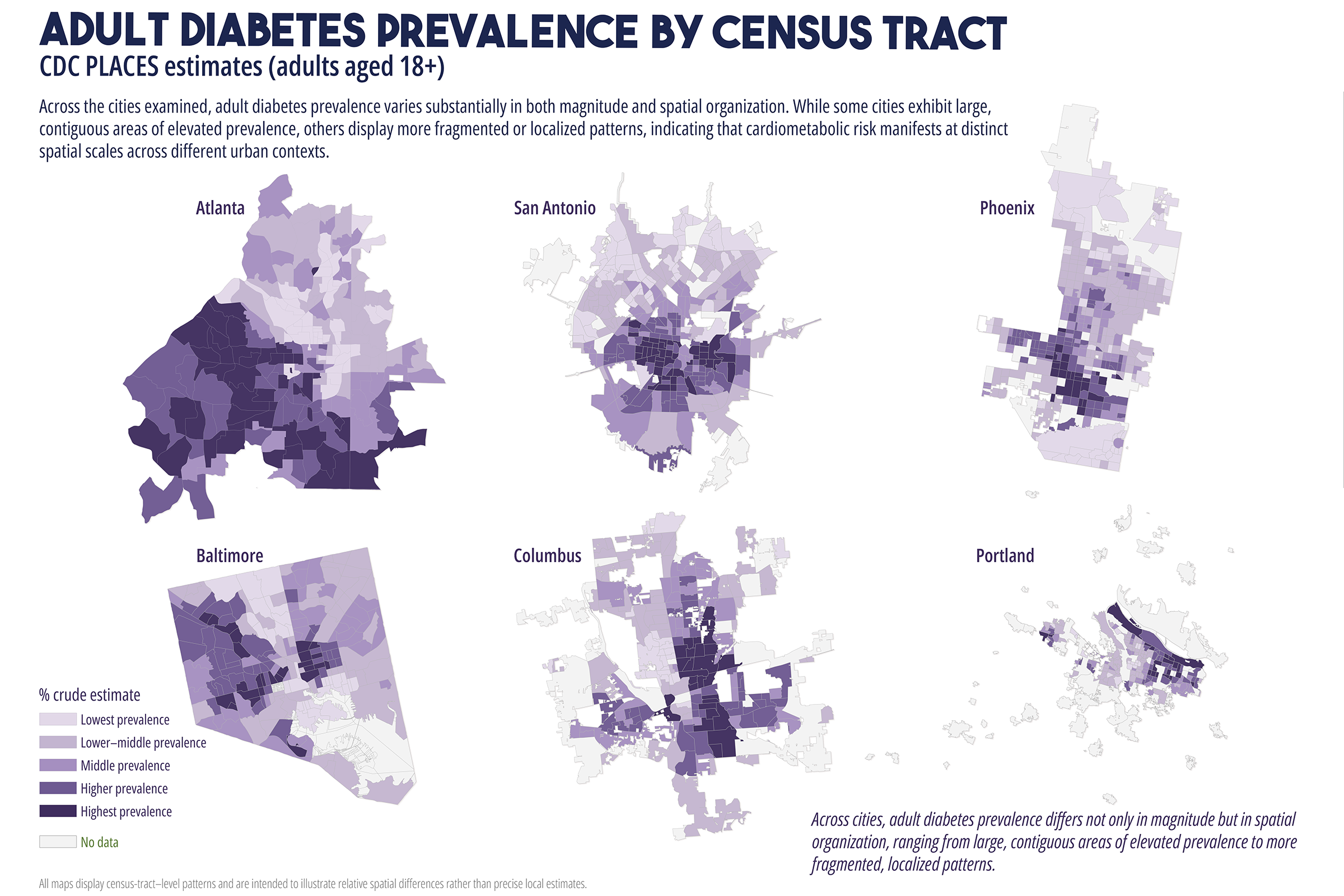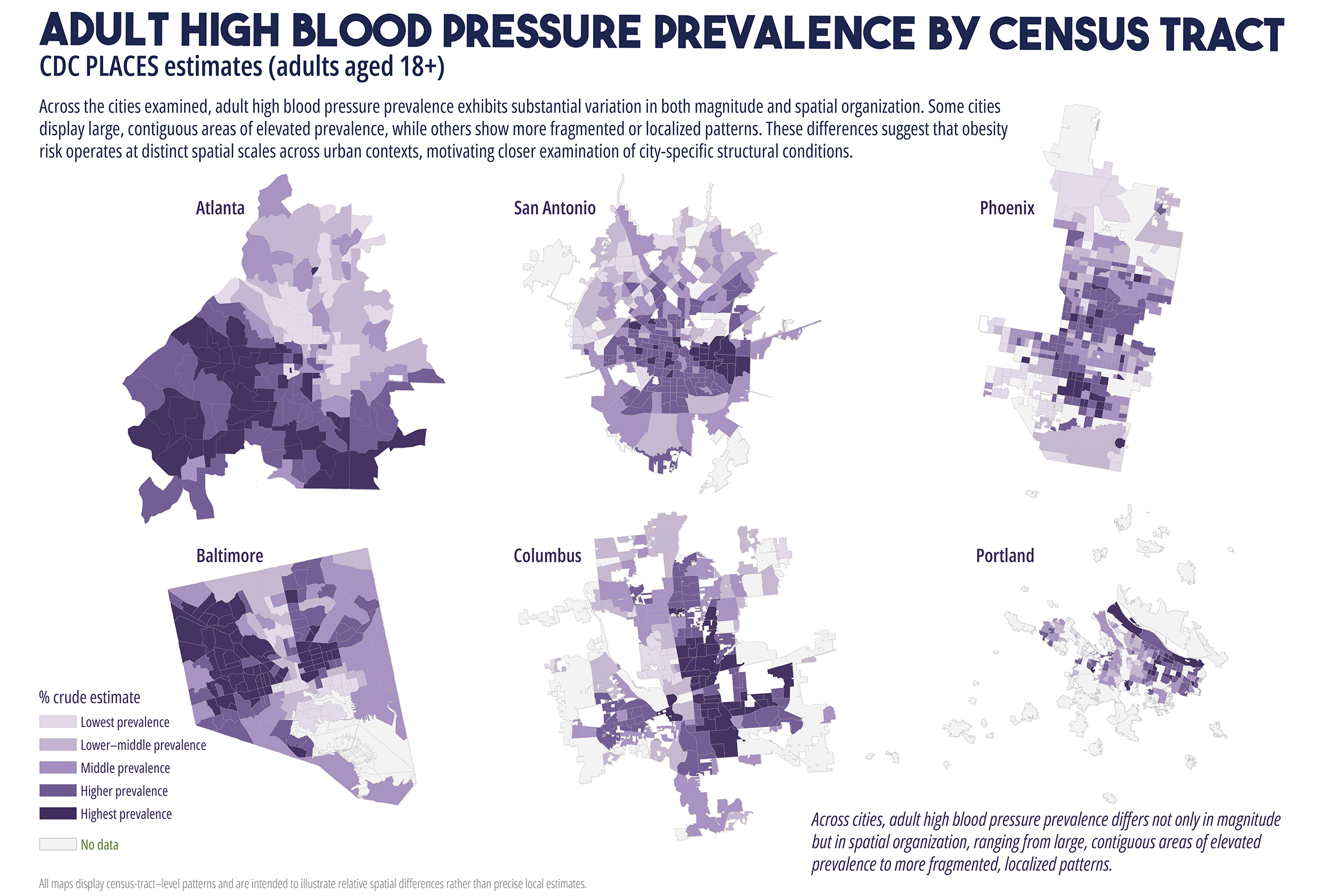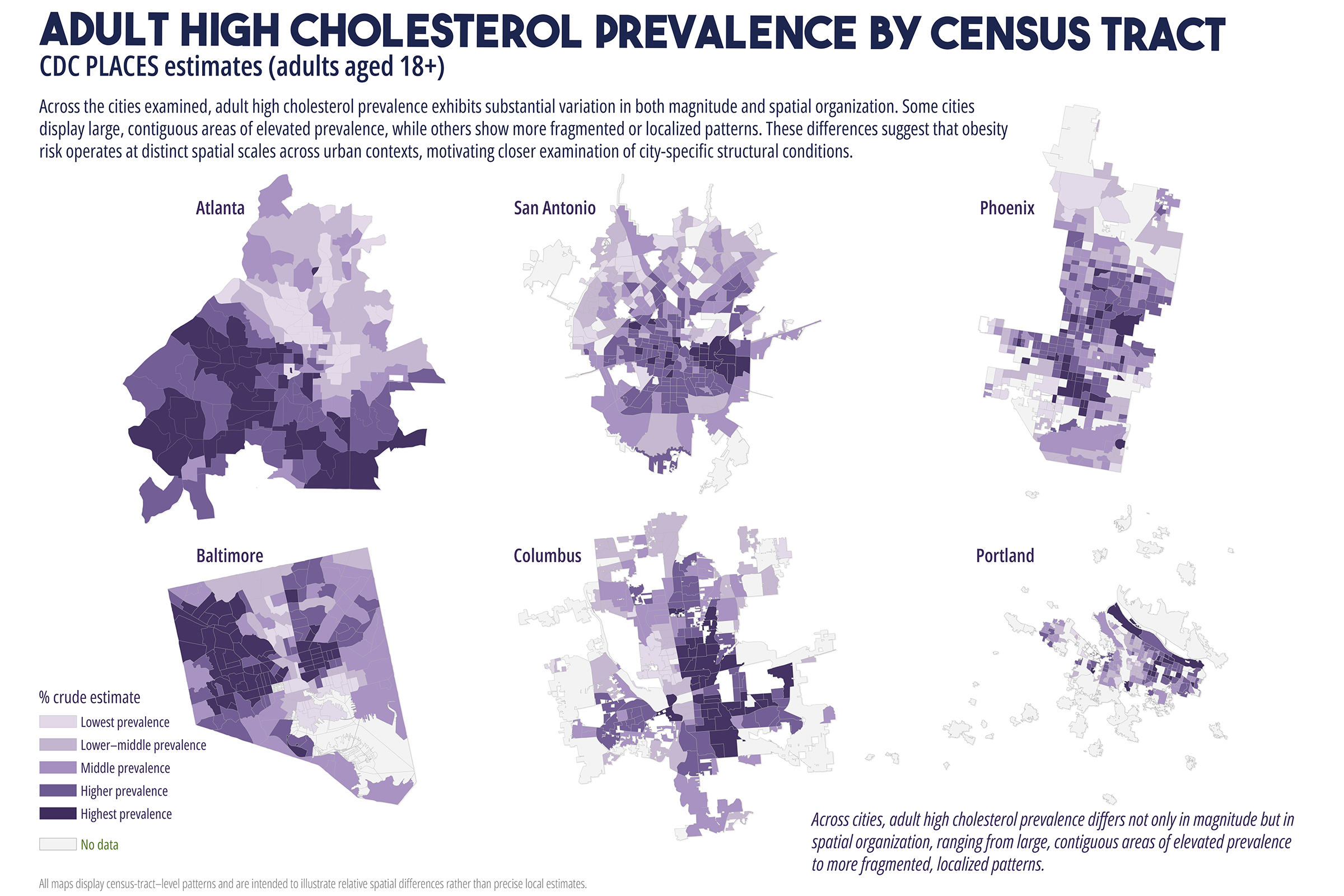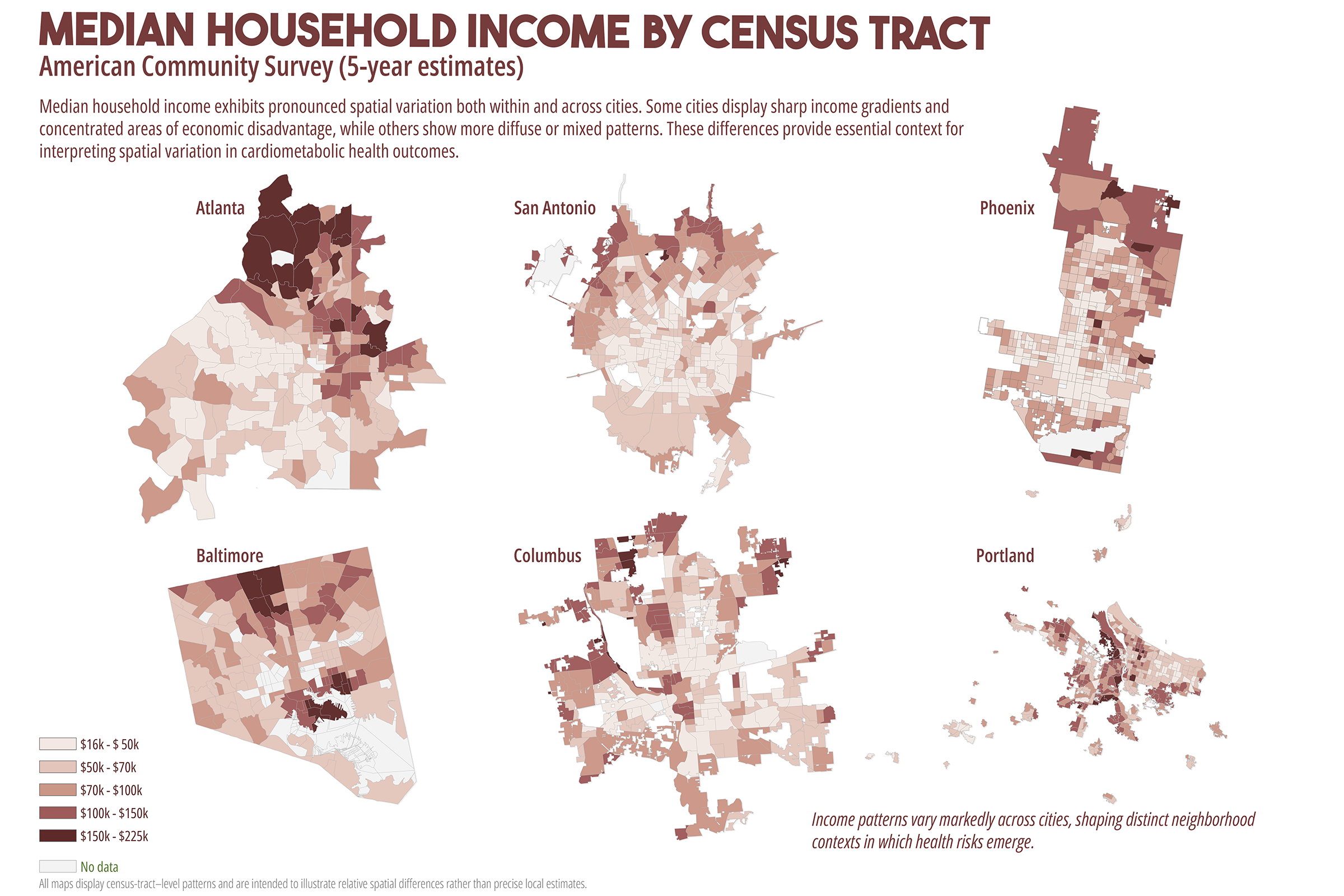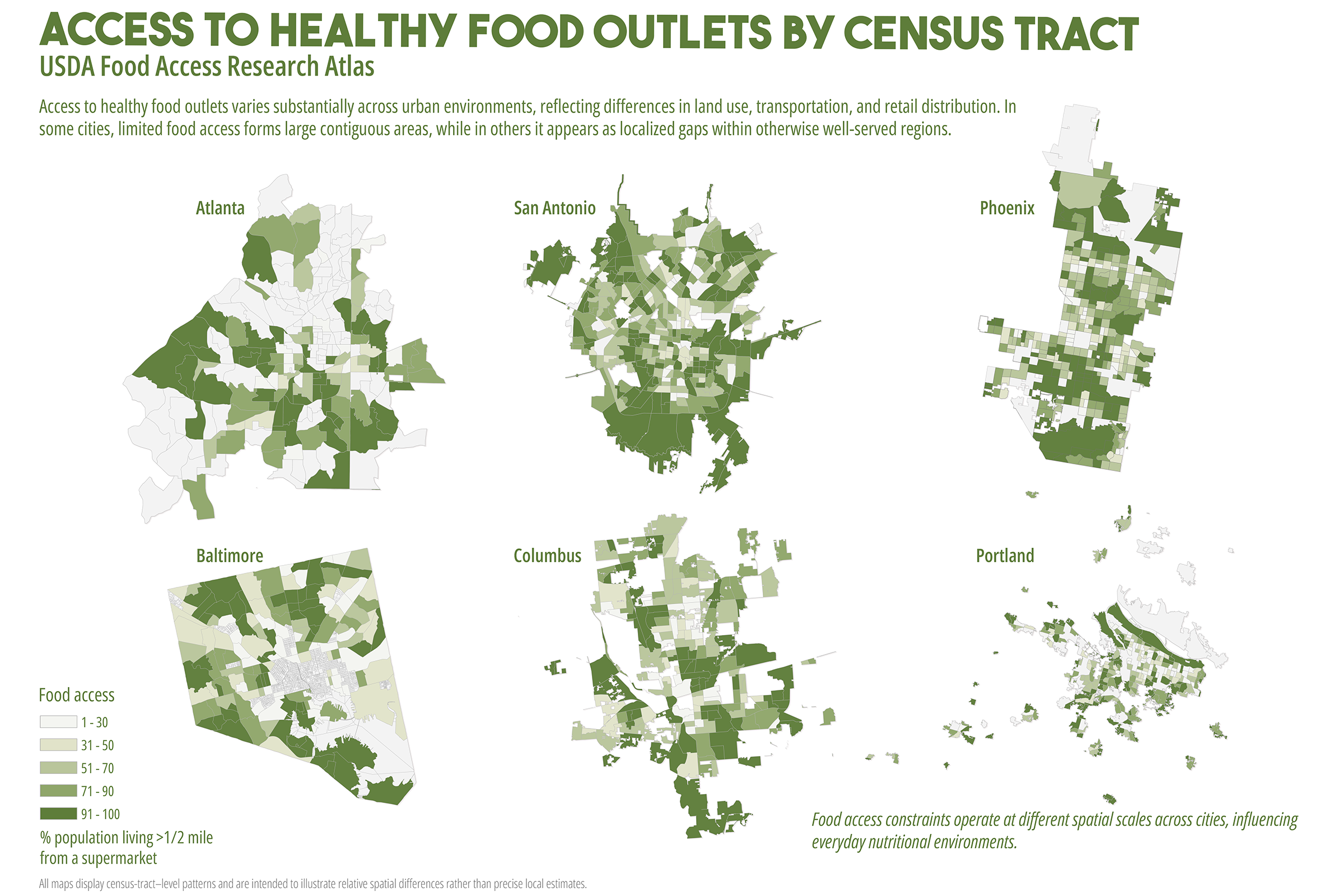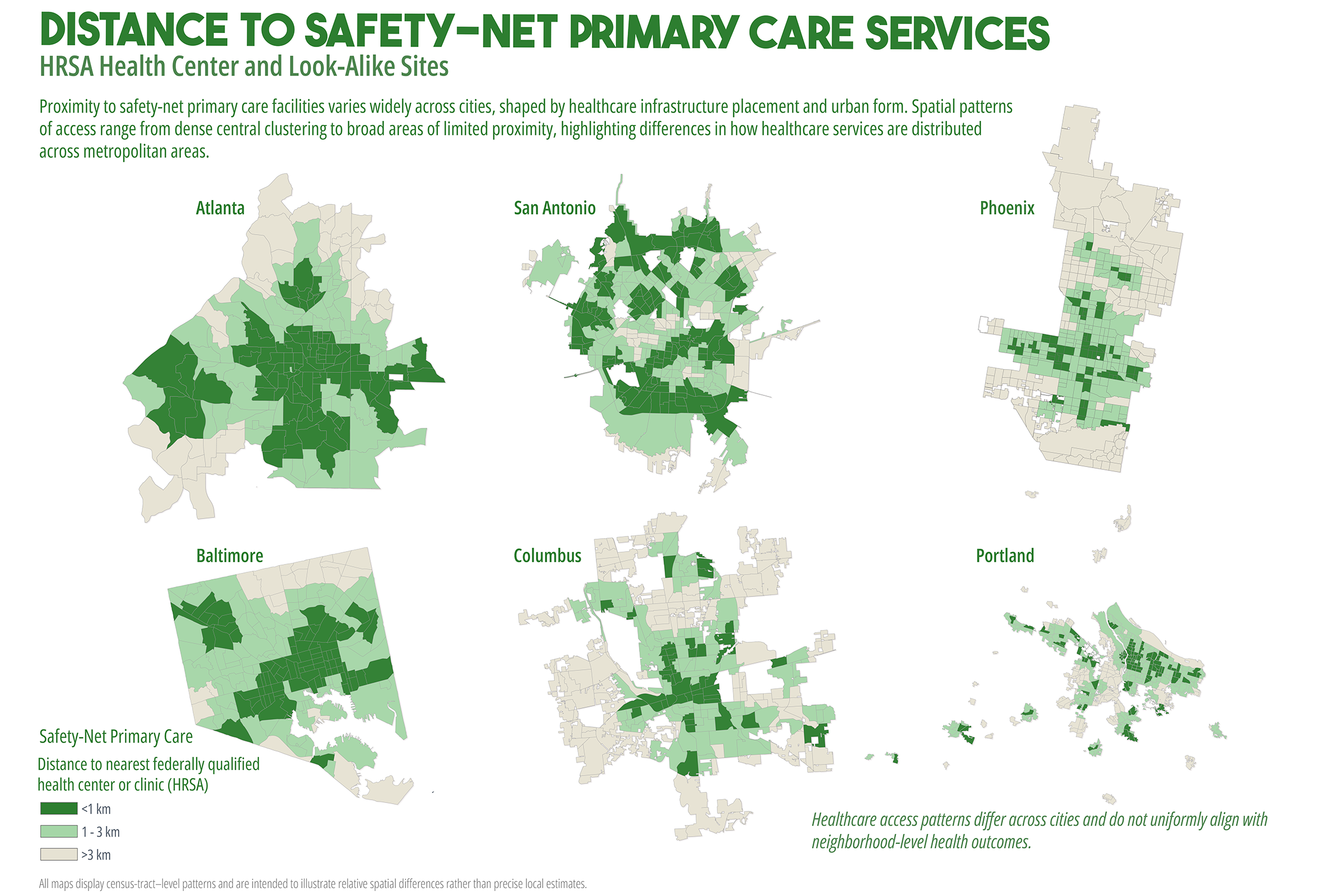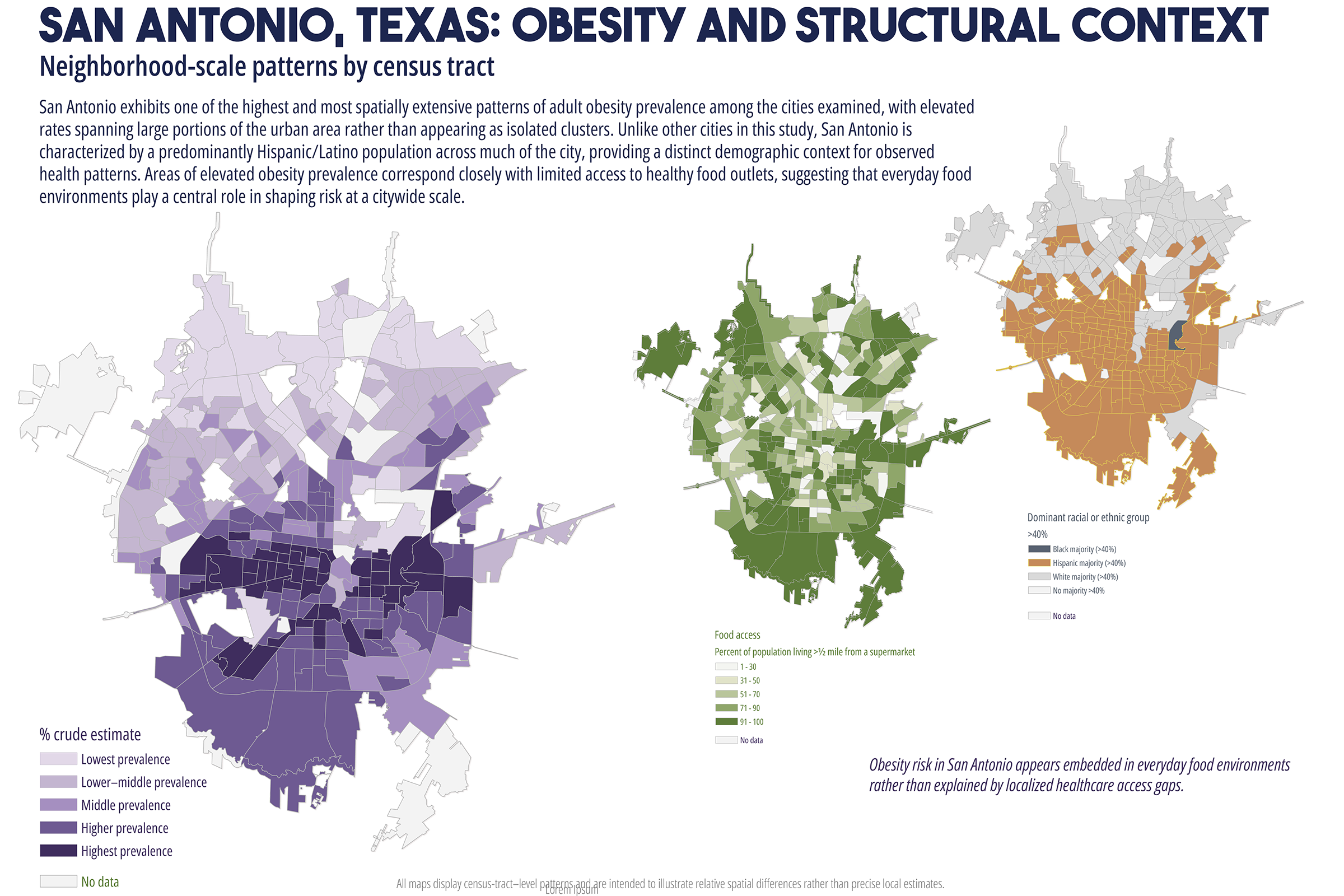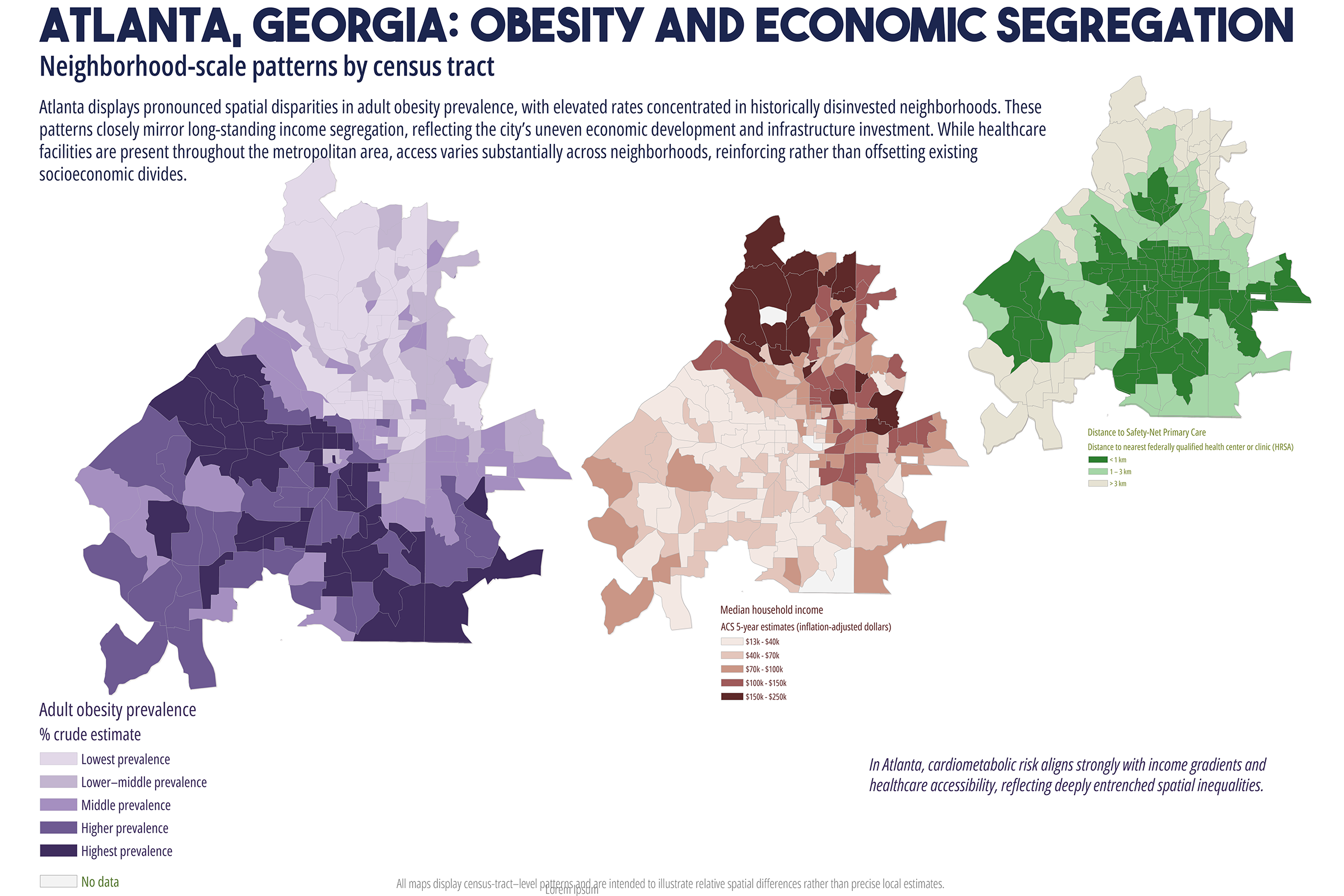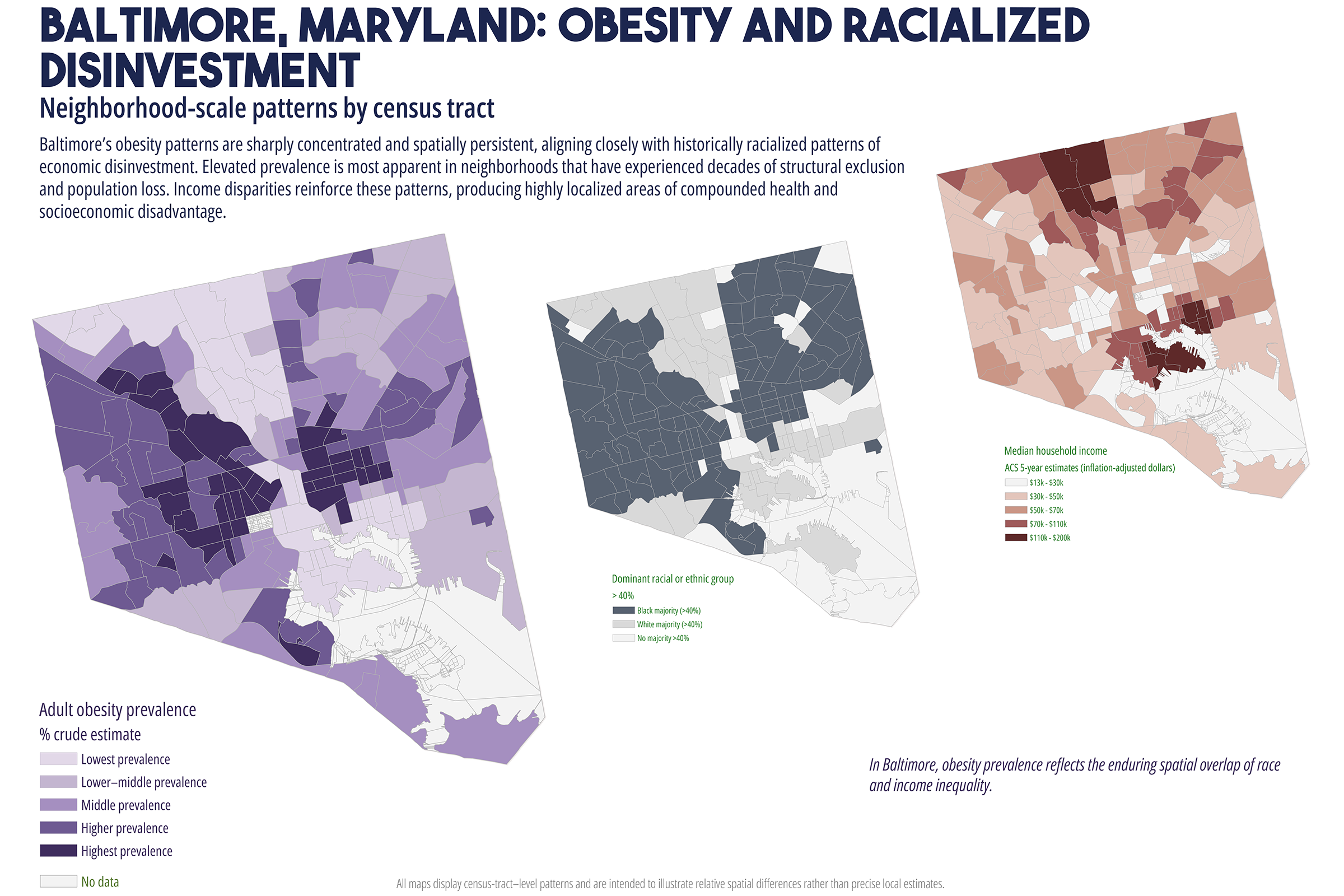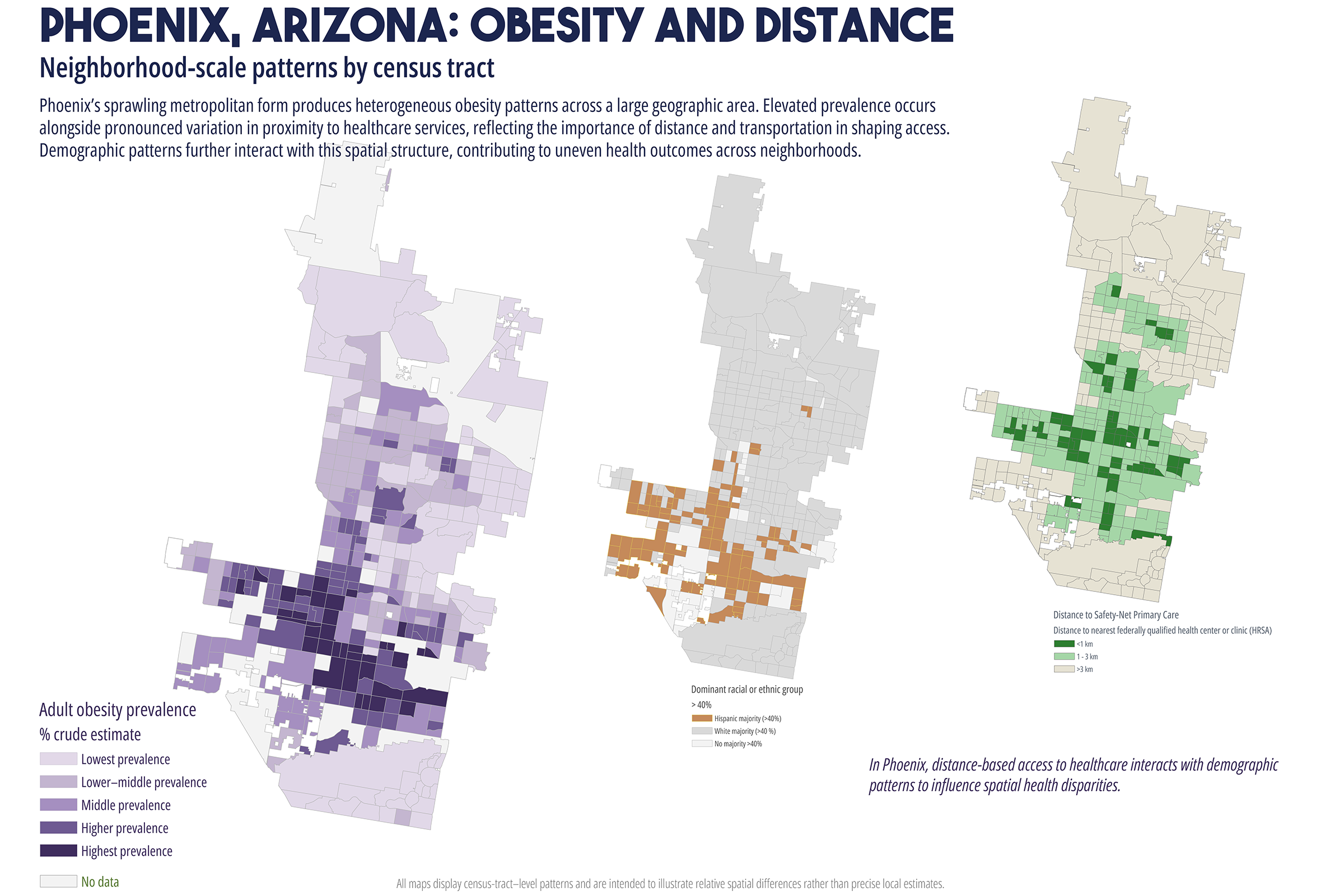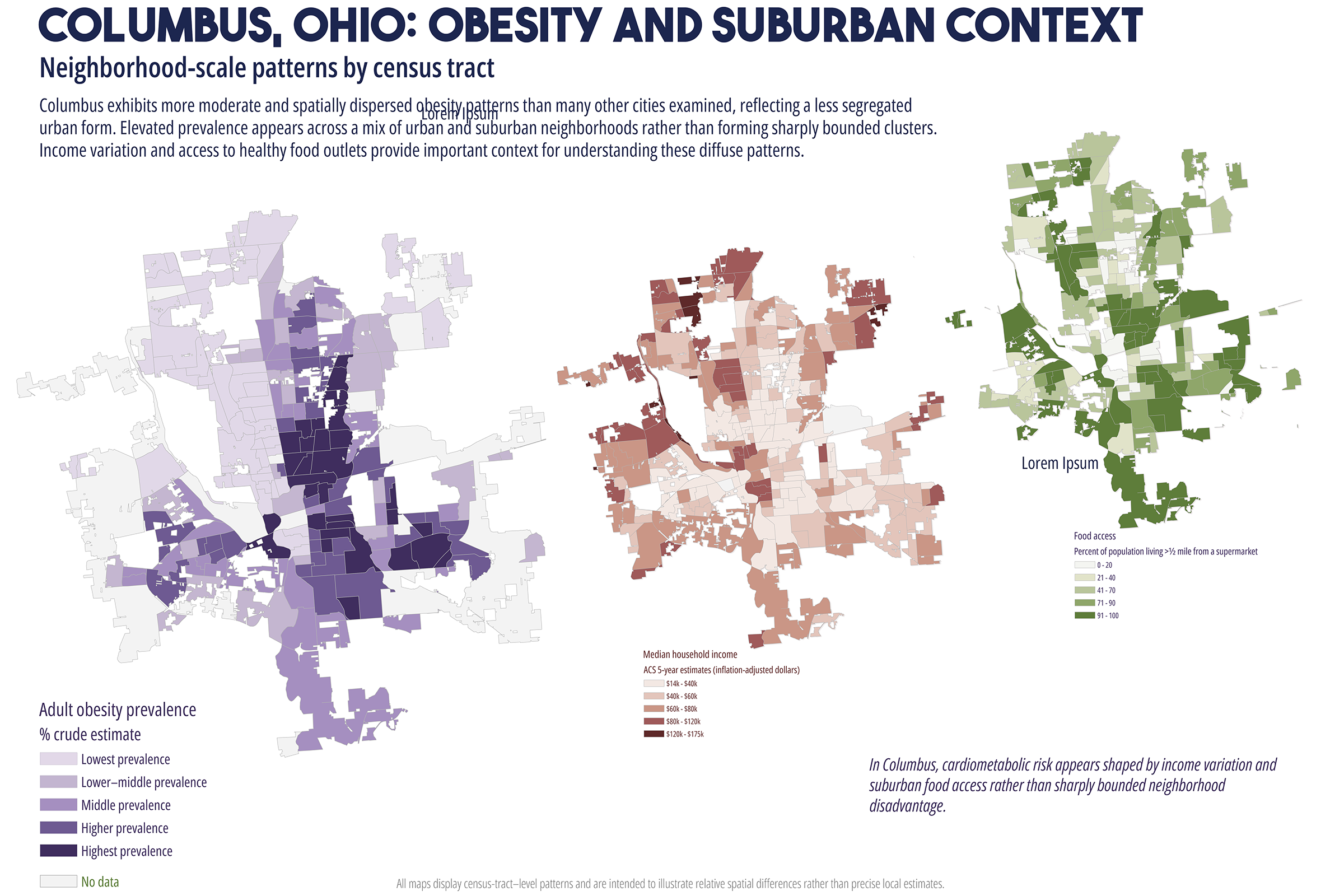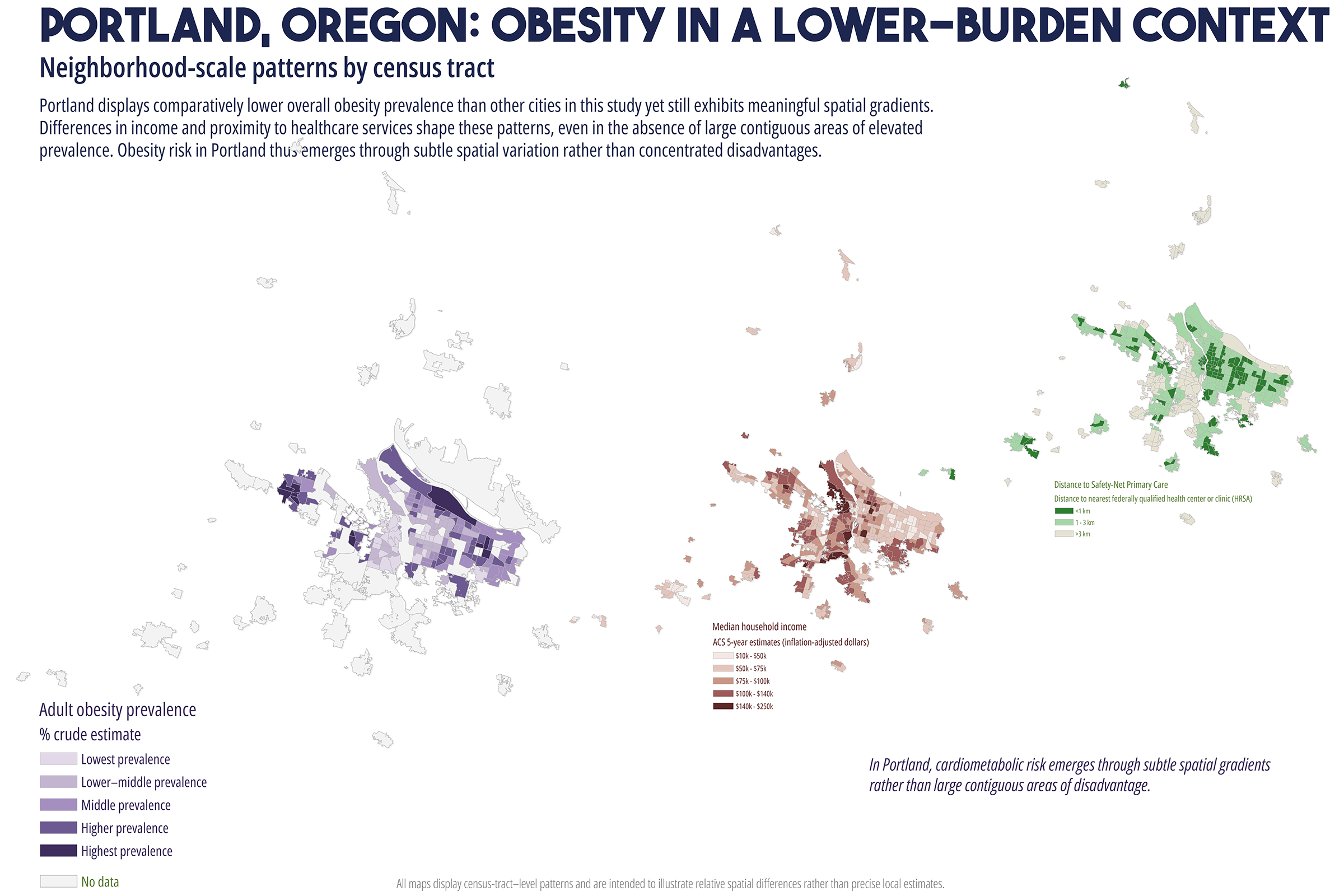

Cardiometabolic conditions, including obesity, diabetes, hypertension, and high cholesterol, exhibit persistent geographic disparities across U.S. cities. These disparities are frequently attributed to unequal access to healthcare, healthy food, education, and socioeconomic opportunities. While relationships are well documented, less is understood about why identical health indicators manifest in markedly different spatial forms across cities, even when measured using consistent data sources and analytic methods. This study employs a comparative, place-based framework to examine census tract-level patterns of cardiometabolic health in six U.S. cities: Atlanta, Baltimore, San Antonio, Columbus (Ohio), Phoenix, and Portland. Using modeled prevalence estimates from the Centers for Disease Control and Prevention (CDC) PLACES dataset, the analysis integrates median household income, dominant racial or ethnic composition, educational attainment, health insurance coverage, and spatial measures of food and healthcare access. By maintaining constant indicators across cities, the study isolates urban context as a central factor shaping health geographies. Results reveal distinct spatial typologies of cardiometabolic burden, including polarized segregation, diffuse majority, corridor-based, growth, and climate related stress patterns. These typologies do not align consistently with access-based metrics alone. In several cities, elevated cardiometabolic prevalence persists in areas with relatively favorable access to food retailers or healthcare facilities, while some low access areas do not exhibit equivalent health burdens. The findings support a constraint-based framework emphasizing lived experiences, chronic stress, environmental exposure, and institutional context as pathways between structural conditions and health outcomes. The paper concludes by discussing implications for urban health policy, arguing for place specific interventions that reduce structural friction rather than relying solely on access expansion or information-based strategies.
Cardiometabolic diseases represent one of the most significant public health challenges in the United States, both in terms of population prevalence and long-term healthcare costs. Conditions such as obesity, diabetes, hypertension, and high cholesterol are strongly associated with morbidity, mortality, and quality of life, and they exhibit pronounced geographic disparities across and within cities (Marmot, 2005; Krieger, 2011). These disparities are commonly framed through the lens of access: to healthcare, to healthy food, to education, and to socioeconomic opportunity. Access based explanations have shaped much of contemporary urban health policy, motivating interventions such as expanding healthcare facilities, incentivizing grocery store development, and implementing community-based health education programs (Thornton et al., 2019).
While these interventions are necessary and often beneficial, their effectiveness has been uneven. In many urban contexts, the burden of cardiometabolic disease remains spatially persistent despite improvements in access to care (Cummins et al., 2014; Conrey et al., 2022). This persistence raises a central question: why do similar cardiometabolic health indicators produce different spatial patterns across cities, even when measured using consistent data sources and methods? Addressing this question requires moving beyond single city analyses and beyond access as a singular explanatory framework. This study adopts a comparative, multi-city approach to examine cardiometabolic health geographies across six U.S. cities with diverse demographic compositions, urban forms, and historical development trajectories. By holding health indicators and analytic methods constant across cities, the analysis employs urban context as a key factor shaping how disease burden is distributed spatially (Diez Roux, 2001; Macintyre et al., 2002).